Breast Revision Gallery





Warning:
This gallery contains nudity. Please click OK to confirm you are at least 18 years of age and are not offended by this material.
Ok
The best time to get your desired breasts is at your very first breast augmentation surgery. The next best time is at the first revision. With each subsequent revision, it becomes less likely that a perfect outcome is achievable.
Having delivered countless breast revision surgeries in Los Angeles, Dr. Teitelbaum regularly fixes the most difficult of all augmentation problems, many of which other plastic surgeons tried unsuccessfully to repair if they were even willing to try at all.
Related Pages on Breast Revision
Dr. Teitelbaum was the very first surgeon to create a classification system to evaluate the complexity and treatment options for correcting horrible breast deformities. Dr. Teitelbaum is an expert in doing breast revision—from simple saline deflation to the most complex cases that simultaneously involve implant malposition, capsular contracture, breast implant rupture, and droopiness.
Many of our Los Angeles breast revision patients are women who are thrilled with their augmentation and just want to do a "tweak" to make breasts they already love even better. This might be changing from saline to silicone, selecting a different size, replacing a very old breast implant with a new one, treating a deflated saline implant, changing size after a pregnancy, or perhaps doing a small breast lift to correct the effects of gravity.
Unfortunately, there are many patients who are emotionally and sometimes physically devastated by previous breast surgery. These patients require a thorough, careful, thoughtful, and technically exacting approach. Each revision operation involves more recovery, money, and anxiety. Oftentimes, scarring and tissue damage from each surgery can make it even more difficult to achieve an ideal result. That all means that it is very important to make sure that the revision surgery is done properly. Dr. Teitelbaum fixes the most complicated of all breast implant problems on a weekly basis. Patients fly in to see him from around the country and frequently from overseas.
He has developed a system to categorize augmentation revision problems, breaking down every problem a patient is having to its component causes, such as issues with their skin, tissue, rib cage, implant, etc. His many videos explain his approach to many breast augmentation problems, and his before and after photos of the Los Angeles breast revisions he has performed demonstrate that he is indeed a breast revision surgery expert.
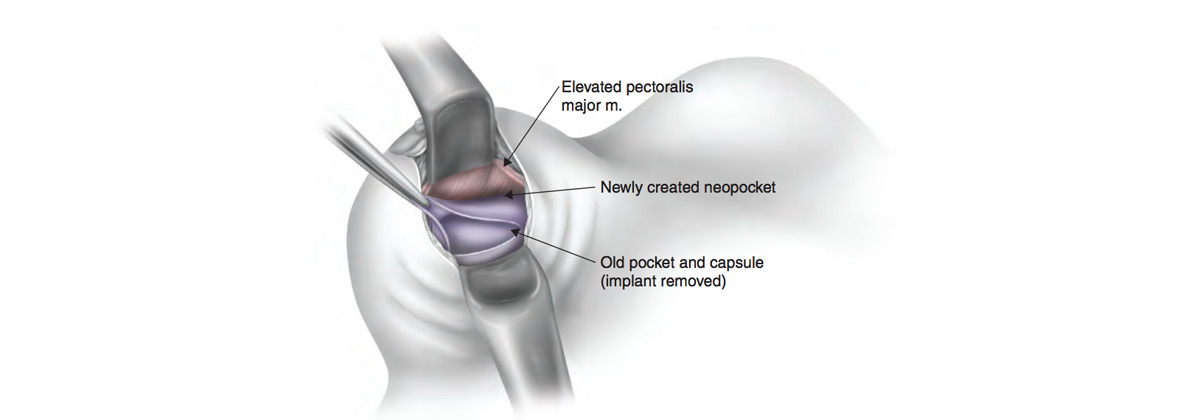
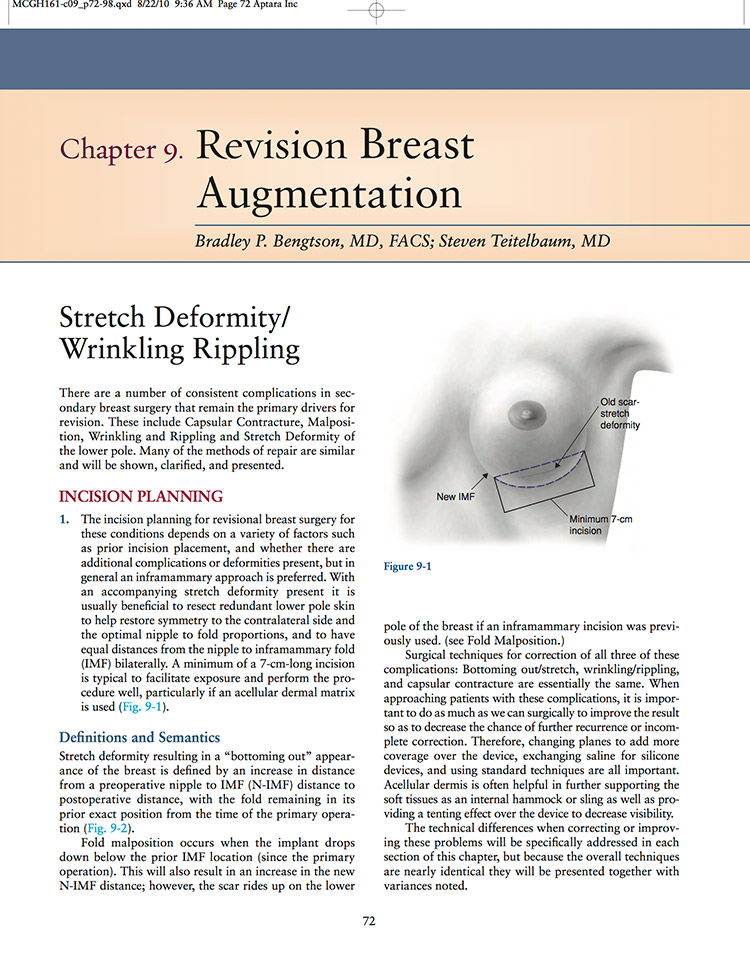
Dr. Teitelbaum has co-authored a chapter which includes a significant description of how to fix rippling.
This 33 page chapter received this comment from the book reviewer: "...one of the most thorough and well considered that I have read on this difficult topic.
Dr. Teitelbaum was a member of this elite panel of surgeons which created algorithms to help surgeons manage important issues in breast augmentation.

When scar tissue in the capsule that cradles the implants hardens around the breasts, this is called capsular contracture. It is a complication that can distort implant appearance, and also be somewhat uncomfortable or painful. There is no known cause for this condition, but, in the hands of a skilled physician such as Dr. Teitelbaum, it can be treated. When the capsule is removed, it's called a capsulectomy.
There are ways that the risk of capsular contracture can be minimized, and Dr. Teitelbaum takes great care to apply these methods carefully during both his primary, revision and capsular contracture treatment surgeries. Using textured implants in a subglandular position may stall capsular contracture because the varied surface will interrupt hardening of the scar tissue. However, this method can result in an implant that may look slightly unnatural. It is a process of balancing the pros with the cons.
In general, placing the breast implants submuscularly has the best odds for avoiding capsular contracture in the first place. In fact, the risk is lowered by up to 12%.
Although studies have been inconclusive as to whether breast massage deters capsular contracture, Dr. Teitelbaum believes it "can't hurt and might help". If anything, massaging the breast tissue will help soften and relax the muscles, allowing the breast implant to settle into place a little faster and more easily.
The "Hands-off" technique is a large part of Dr. Teitelbaum's approach when handling breast implants during his breast revision surgeries. He carefully opens the sterilized implant container only at the moment of insertion, and no one else handles the implants except the doctor. The breasts are rigorously sterilized, and both dressings and gloves are meticulously changed at every juncture to ensure the treatment area is immaculate at all times. This fastidious attention to detail significantly lowers the likelihood of germs or foreign bodies entering the breast cavity, which may lead to capsular contracture if allowed to seep through.
Meaning "bad position," malposition is a general umbrella term that covers a range of implant problems, most highly correctable. Implants may land too low, high, medial or lateral. While most issues will be reversed surgically, Dr. Teitelbaum may suggest a non-surgical tactic as well if the case permits it.
This condition can be caused by improper placement of the underlying capsule, or a breast implant that has simply not settled down into its correct position. Another cause is noted to be that the patient may have worn an underwire bra too early in their recovery, which may have unwisely elevated the implant and prematurely sealed the implant pocket that was supposed to stretch with time. Finally, capsular contracture may also result in an implant that appears too high, when the lower part of the breast chamber hardens, forcing the implant to migrate upwards.
This unfortunate condition is also dubbed bottoming out or double bubble. Sometimes the capsule was created in the wrong place by an inferior surgeon, while other times the breast implant just migrates downwards of its own accord. A common cause is a lack of proper support at the breast crease (a lack of appropriate inframammary attachments). In general, those clients seeking larger implants tend to have this problem the most.
Implants that have migrated laterally can look quite unsightly, but Dr. Teitelbaum has the tools and skill to correct such error during a breast revision in Los Angeles. Sometimes this condition is caused by ill-formed breast pockets, or it is due to a lack of strong attachments that might keep the implants from shifting towards the armpits. Rib placement can also play a role, as when they bend towards the back, the implants may follow. Lastly, some clients may find that stomach sleeping worsens the tendency of the implants to widen.
Symmastia occurs when the implants appear too squashed together, huddled near the middle of the chest. Sometimes the nipples will face outwards, which is given the nickname "walleyed". This error can be traced back to improper capsule formation. While mostly cosmetic, symmastia can also cause discomfort for the patient and should be corrected by a skilled, patient and dedicated surgeon who has ample experience in this area of medicine.
Yes. A skilled surgeon can refine the breast pocket, adjust implant type or placement, and even use fat grafting to soften the transition and create a more natural contour. The goal is to restore balance and proportion—enhancing your results without compromising safety or structure.
Most surgeons recommend waiting at least 6 to 12 months before pursuing revision surgery. This allows swelling to subside and tissues to settle, giving a clear picture of your final outcome. However, if you experience discomfort, implant rupture, or significant asymmetry, an earlier evaluation may be appropriate.
Absolutely. Over time, natural aging, pregnancy, or weight changes can affect breast position, firmness, and symmetry—even with implants in place. Revision surgery can restore a youthful contour by tightening tissue, repositioning implants, or combining a lift with replacement for refreshed, natural-looking results.