Before & After




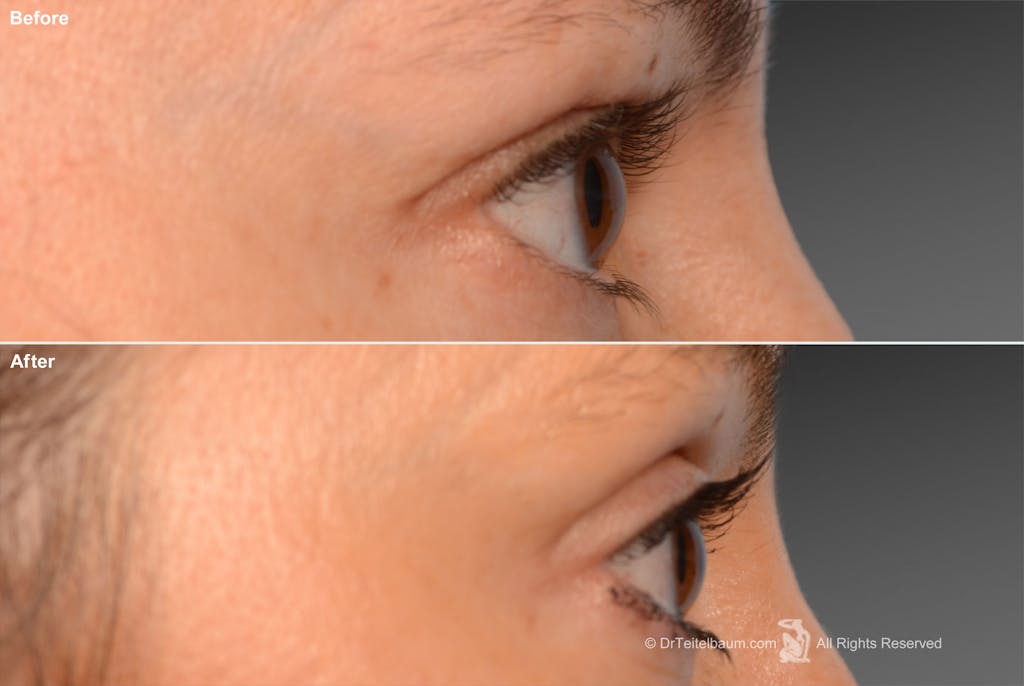

The eyes are the most expressive feature of the face. They communicate vitality, emotion, and health more than any other facial feature. Even subtle changes to the eyelids can make someone appear tired, aged, or unwell—while thoughtful eyelid surgery can restore a refreshed, natural appearance without looking “done.”
Dr. Steven Teitelbaum is a board-certified plastic surgeon in Santa Monica and Los Angeles with decades of experience performing eyelift surgery designed to enhance the eyes while preserving their essential function and natural character.
An eyelift, also known as blepharoplasty, and eyelid surgery is a surgical procedure that improves the appearance of the upper eyelids, lower eyelids, or both. The goal is not to change the shape of the eyes, but to restore balance by addressing excess skin, bulging fat, or laxity that develops with age or genetics.
Eyelid surgery can:
Because the eyelids frame the eyes, even small refinements can create a significant improvement in how rested and youthful the face appears.
Upper eyelid concerns are among the most common reasons patients seek facial surgery. Excess skin on the upper lids can make the eyes look tired, interfere with makeup application, and cause people to unconsciously raise their brows, leading to horizontal forehead lines.
An upper eyelift removes only the necessary amount of skin and, when needed, small amounts of fat. Dr. Teitelbaum is meticulous about avoiding overcorrection, as removing too much skin can lead to a hollowed or unnatural appearance and affect eyelid closure.
Upper eyelift surgery:
Incisions are placed in the natural eyelid crease, where scars typically heal exceptionally well and are difficult to detect.
Lower eyelid aging most often presents as bulging fat rather than excess skin. These under-eye bags are frequently genetic and can appear even in younger patients.
In most cases, Dr. Teitelbaum performs a transconjunctival lower eyelift, removing or repositioning fat through an incision hidden inside the eyelid. This approach:
When mild skin laxity is present, a very conservative skin pinch may be added. Dr. Teitelbaum is careful to maintain fullness and support of the lower lid, avoiding the hollowed or pulled-down appearance that can occur when too much skin or fat is removed.

The eyelids and eyebrows function as a unit, and no eyelift plan is complete without evaluating brow position. A low brow can make the upper eyelids appear heavy, while a well-positioned brow can significantly reduce eyelid hooding.
In general:
Some patients benefit from both procedures, while others need only one. When both are performed together, precise judgment is required to balance brow elevation with eyelid skin removal. In certain cases, Dr. Teitelbaum may recommend staging procedures to ensure safety, natural appearance, and proper eyelid closure.
Eyelid surgery is often performed alone, but it is commonly combined with a facelift. A facelift rejuvenates the cheeks, jawline, and neck, while an eyelift refines the eye area—ensuring harmony across the entire face.
When performed together:
Conversely, many patients who do not wish to undergo a facelift can still achieve dramatic, natural improvement with eyelid surgery alone.
The negative stereotypes associated with eyelid surgery almost always stem from overcorrection. Dr. Teitelbaum believes eyelift surgery should enhance the eyes without drawing attention to itself.
His approach emphasizes:
Contrary to popular belief, the “surprised” or “deer in headlights” look is caused by overly aggressive brow lifting, not eyelid surgery. By elevating the brow conservatively and refining the eyelids with restraint, Dr. Teitelbaum produces results that look refreshed, expressive, and natural.

You may be a good candidate for eyelid surgery if you:
A consultation allows Dr. Teitelbaum to evaluate whether an eyelift, brow lift, or combination of procedures will best address your concerns.
Recovery from eyelift surgery is generally straightforward.
Most patients experience mild swelling and bruising
that improves steadily over the first week.
Typical recovery milestones include:
Dr. Teitelbaum prioritizes careful planning and conservative technique
to minimize downtime and protect eyelid function throughout recovery.


Dr. Teitelbaum’s lifelong exposure to ophthalmology, artistic background, and decades of surgical experience uniquely position him to perform eyelid surgery with exceptional judgment. His focus on anatomy, function, and aesthetics allows him to deliver results that enhance the eyes without compromising comfort or expression.
He achieves an improvement that is dramatic yet does not specifically draw attention to itself. Skin needs to be removed, fat may need to be removed, and wrinkles smoothed. It is all too common to see when the eyes are deprived of fat or the eyelids are deficient in skin.
Dr. Teitelbaum performs his eyelift surgeries so that his patients’ eyes can be front and center, neither being concealed by the eyelids nor looking “bug-eyed.” He is an expert at avoiding surgical telltales, and will create a look that is harmonious and balanced with your face.
Dr. Teitelbaum has performed eyelids with great interest since he was a resident. His father is an ophthalmologist and he benefited from a lifetime of learning and understanding about eyes.
He has since performed hundreds of eyelid surgeries of all sorts, on their own, with laser treatments, with brow lifts, and with facelifts. His command of the anatomy of the eye, appreciation of the important function of the eyelids, and fine aesthetic sensibilities enable him to consistently produce beautiful eyelid results.
Yes. A natural-looking eyelift focuses on removing only the necessary skin or fat while preserving eyelid function and fullness. Dr. Teitelbaum is careful to avoid overcorrection, which is what creates a hollowed or surgical appearance.
An eyelift improves the appearance of the eyelids but does not change the fixed shape of the eyes. The eyes may look more open and refreshed, but their natural structure remains the same.
Some patients use less Botox after an eyelift because excess skin is no longer weighing down the lids. However, Botox may still be used to soften forehead lines or crow’s feet, depending on individual needs.
If dark circles are caused by bulging fat that creates shadows, an eyelift can improve their appearance. However, pigmentation-related dark circles are not corrected with eyelid surgery.
The skin and fat removed during an eyelift are permanently removed. Most patients never require another surgery, though minor adjustments years later are occasionally requested.
Revision eyelid surgery is rarely needed. When it is, the main concern is ensuring enough skin remains for proper eyelid closure. Dr. Teitelbaum’s conservative approach helps preserve future options.
Lasers can improve fine wrinkles and skin texture but cannot remove excess skin or bulging fat. Eyelid surgery and laser treatments address different concerns and are sometimes used together.
In rare cases, insurance may cover an eyelift if excess skin obstructs vision and proper documentation is provided. Most eyelift procedures, however, are considered cosmetic.
