Breast Revision Malposition Gallery





Warning:
This gallery contains nudity. Please click OK to confirm you are at least 18 years of age and are not offended by this material.
Ok
If an implant is not properly positioned behind the breast, the breast will look very odd. If the breast implant is too high, there will be an upper bulge and the nipple will tip down. If they are too close together, the skin will tent over the breastbone and the breasts will look like they are joined together, a condition called symmastia (or “uniboob”).
If the implants are placed too low, the upper breast will be empty and the nipples will tip up. If they are placed too far out to the sides, cleavage will be absent and the nipples may tip inwards. The beautiful breast has the proper ratio of volume above and below the level of the nipple, as well as to the inside and outside of the nipple.
With Dr. Teitelbaum’s expertise in treating malposition in Los Angeles, he has corrected every type and every combination of these deformities, has written articles on it, and has taught new techniques for correcting them to many surgeons. One technique closes off the unwanted portion of the pocket in which the implant sits (“the capsule”) with special stitches; this is called a “capsulorrhaphy.” Another technique is the “neosubpectoral pocket” or “neosubglandular pocket”. This is a new technique which Dr. Teitelbaum has written about and taught to other surgeons, and it is based upon using the body’s own tissues to close off the pocket. If there is an instance when tissue is weak, Dr. Teitelbaum can reinforce it with an acellular dermal matrix (ADM), such as AlloDerm or Strattice. In other cases repairs can be reinforced with an artificial mesh, such as Seri Scaffolding or Galaflex.
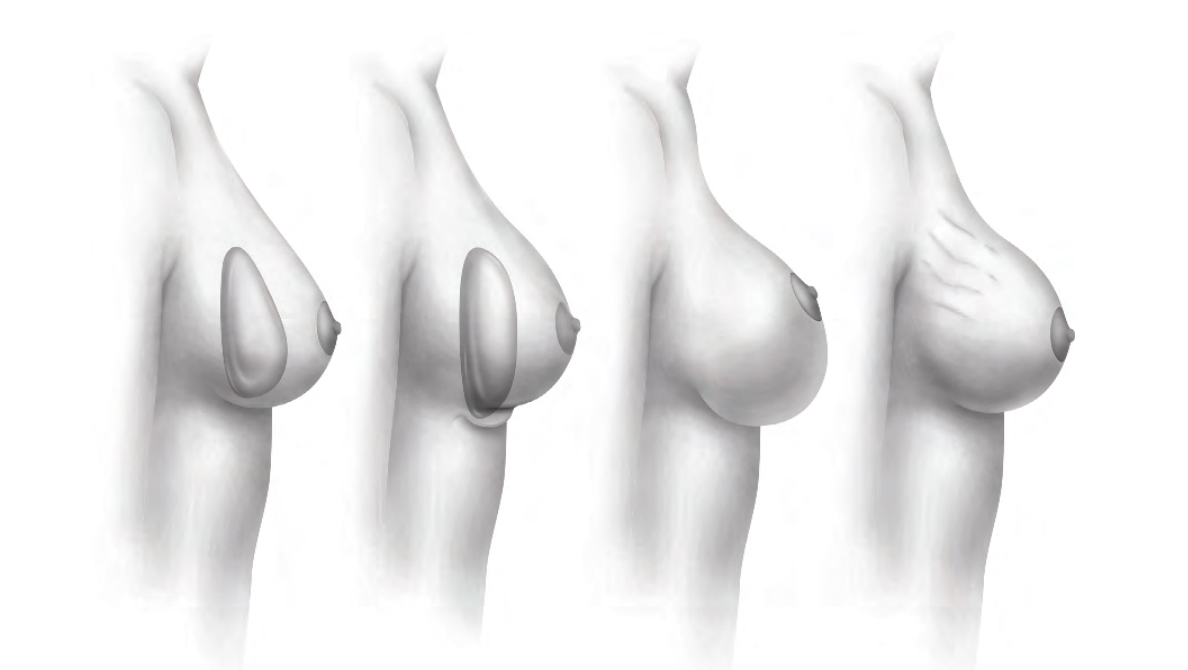
This illustration from one of Dr. Teitelbaum’s book chapters demonstrates the difference between three closely related problems: fold malposition, stretch, and rippling.
When a breast implant falls too low there will be too much breast volume beneath the nipple and not enough above the nipple. The empty upper breast allows the nipple to point up too high. If the scar for insertion was underneath the breast, it may appear to rise up onto the lower pole of the breast. Not only is this unattractive, but in these circumstances the nipple may occasionally rise up and out of a bra. And when an implant is low, the breast appears low on the torso, making the abdomen look more low and square. This situation can arise from a less-than-excellent surgery, but it can also occur after perfect surgery if the patient’s tissues are not strong or if a heavy implant is gradually pulled down by gravity.
When a low implant falls beneath a tight “inframammary fold”—the crease that defines the bottom of the breast—a so-called “double-bubble” deformity can occur. This is due to there being a layer of breast tissue above the original fold, and the absence of breast tissue beneath it. So when the implant is lower than that original crease, a hump can appear on the lower surface of the breast, which is what is called a double-bubble.
While an inferior malposition can occur in isolation, it can often occur with implants simultaneously being misplaced out to the side or towards the center.
Inferior malposition is fixed either by reducing the size of the existing pocket holding the implant or by creating a new pocket with a procedure called a neosubpectoral pocket, which Dr. Teitelbaum has published on and taught to many other surgeons. When the tissues are weak—as they sometimes are with inferior malposition—they can be strengthened with the use of something called Acellular Dermal Matrix (ADM), which is a sheet of collagen used to reinforce tissue. A mesh such as Seri Scaffolding or Galaflex can also help in some situations. As a top Los Angeles treatment specialist for bottoming out, double bubble, and the so-called “uniboob,” Dr. Teitelbaum regularly sees patients from around the world who have already suffered from this problem and unsuccessful attempted correction procedures.

When a breast implant is high, there is often too much volume above the nipple and not enough below it. The bottom of the breast will be empty and the nipple will point downwards. There will be an upper bulge that can be severe enough to create a shelf. Also, the upper breast gets an overly demarcated edge and becomes round and obviously augmented. Patients will complain that their breasts look fake and that their nipple position looks odd even through clothing. A number of factors can contribute to an upper implant malposition in Los Angeles, and fortunately, this is one of the most straightforward breast implant revision procedures.
In some circumstances, the initial surgeon did not determine the proper position for the bottom of the implant, so that it never sat in the proper position relative to the patient’s own breast mound and nipple. The pocket made for the implant can sometimes fill with fluid after surgery, fuse together, and force the implant upwards. Sometimes, muscle fibers at the bottom of the breast need to be released in order to allow the implant to sit properly may not have been accurately handled in the original surgery, thereby preventing the implant from falling into the ideal place; while this can happen with any incision, it is more frequently noticed in patients who had their implants placed through the armpit incision. Finally, the development of scar tissue around the implant—capsular contracture—inevitably pulls the implant upwards as it tightens around it.
If a patient recalls that the breast implants looked good after their breast augmentation but later developed a problem, then the likely diagnosis is capsular contracture. That diagnosis is usually confirmed if the implant has gotten harder or more uncomfortable. If the implant was high from the very beginning and never got better, then it is likely that the implant was placed too high or the muscle was not adequately released.

An overly large or highly projecting implant should not be confused for superior malposition. An implant fills the breast from the bottom up, so if an implant is too large there will also be an upper bulge and the nipple will tilt downwards. It is only considered a malposition if the implant does not sit at the bottom of the breast. This is an important point and often overlooked. If you think about it, if a very tiny implant were placed, there certainly wouldn’t be an upper bulge. But if a gigantic implant were placed, it is easy to imagine that there would be a big upper bulge. While that might at first appear to be malpositioned too high, it could be the case that the implant is simply too big.
With inferior, medial, and lateral malposition, the repair must be strong enough to resist the pressure of the implant or gravity. But gravity works in the patient's favor with superior malposition. In cases of capsular contracture, removal of scar tissue fixes the problem. If the problem is too large of an implant, the implant size can be reduced. And if there is tissue under the implant blocking it from falling into the proper location, release of that tissue will allow the implant to settle down lower and into a more ideal position.

When breast implants are too close together, it is called symmastia (or “uniboob.”) This can vary from implants being just a little too close together and tenting up the skin over the breastbone, to implants that are actually touching one another and creating a true uniboob. Sometimes the implants are equally malpositioned, and sometimes one may be in the proper position but the other may cross the center line of the body. It’s good to have cleavage, but with symmastia there is too much cleavage and the cleavage does not look normal or attractive.
Since too much of the breast implant volume is located between the nipples, the nipples are often tipped outward and the breasts can look very deformed. It is very frustrating to women because this is something that oftentimes cannot be hidden with a bra.
Many of the symmastia patients Dr. Teitelbaum sees for malposition in Los Angeles have inferior malposition (breast implant too low) in conjunction with symmastia.
Four basic conditions contribute to the development of symmastia. The first is a depressed breastbone, which allows the implants to fall towards the center when a patient is on their back. In its severe form, a depressed breastbone is called pectus excavatum. This condition is not always symmetrical, so many symmastia patients are uneven. (This is the opposite of pectus carinatum patients, who have overly prominent breastbones, thereby causing their breast implants to be pushed out to the sides.)
The second situation is that the pocket was not accurately dissected. As careful as surgeons know to be when performing breast augmentations, sometimes a surgeon inadvertently makes the pockets too close together. When implants are placed behind the muscle, the muscle attachments on the side of the breastbone are to be left intact; but some surgeons intentionally divide them in an effort to put the implants closer together. This creates a big risk for the implants falling too close together. If an implant is placed in front of the muscle, then there is no natural anatomic boundary for the dissection, and so it is easier for a surgeon to mistakenly make the pockets too close together.

Some surgeons believe that making a big pocket and having patients massage their breasts is a good way to reduce capsular contracture. Though that has shown to be incorrect, some surgeons still do this. If the pocket is opened up too much towards the center then the implants can fall too close together.
The third contributing factor is implant size. The bigger the implant, the more pressure it will place on the surrounding tissue, which can tear or stretch with time. A great many patients have implants that are simply too large for them. They may be too wide for a patient’s rib cage and therefore are essentially forcing themselves towards the center. Or they can be so projecting that as they push the skin forward they tent the skin off of the breastbone.
The last factor is the strength of the patient’s tissues. Some patients have very thick, tight, and strong tissues. Some have thinner and more flexible tissues that are less able to withhold the pressure of an implant and are more susceptible to allowing the pocket to enlarge.
If a patient reports that symmastia existed immediately after surgery, there is a suggestion that the problem was the pocket being made too large. If the symmastia developed later, it probably means that the pocket enlarged by pressure, which would be some combination of implant size and weight, the shape of the rib cage, and the strength of the tissues.
Los Angeles symmastia treatment surgeon, Dr. Steven Teitelbaum, is an expert in breast revision surgery in general, and symmastia in particular. He has treated patients from all around Santa Monica, Los Angeles, Beverly Hills, and even from overseas. He has written an original article on treating symmastia in the most important plastic surgery journal, has published a book chapter teaching surgeons how to do it, and has taught a course on it at the biggest plastic surgery meeting.
There are a variety of techniques for treating symmastia, and no one technique works for all patients. With his experience and expertise in all of the various methods, he can give you your best chance at getting your symmastia corrected. One technique closes off the unwanted portion of the pocket in which the implant sits (“the capsule”) with special stitches; this is called a “capsulorrhaphy .” The method also depends upon whether the implants were in front of the muscle or behind the muscle.
Another technique is the “neosubpectoral pocket” or “neosubglandular pocket”. This is a new technique which Dr. Teitelbaum has written about and taught to other surgeons, and it is based upon using the body’s own tissues to close off the pocket. If there is an instance when tissue is weak, Dr. Teitelbaum can reinforce it with an acellular dermal matrix (ADM), such as AlloDerm® or Strattice, or it can involve the use of a mesh such as Seri Scaffolding or Galaflex. A critical component for many patients is accepting a smaller implant. The best repair in the world cannot hold up against a significant amount of pressure from a large implant. This is something that Dr. Teitelbaum will discuss with you at length in his Santa Monica office during your symmastia consultation.
Nearly every patient who sees Dr. Teitelbaum for a breast augmentation emphasizes that she does not want breasts that are far apart and that she wants as much cleavage as can be attained naturally.
In light of this, patients with implants far out to the sides find the condition to be very distressing. This problem can be the result of making too large of a space for the implants or making the space too far out to the side at the initial breast augmentation procedure.
Widely placed implants can interfere with a patient’s arms, leave too large of a gap between the breasts, or allow the nipples to point inwards from too much outer breast fill and not enough inner breast fill.
Frequently, this malposition is the result of a patient with a breastbone that protrudes too far forward. When these patients lay on their backs, their chest essentially has the shape of the roof of the house, which allows the implant to gradually slip outward along the sides of her chest. A large or heavy implant and weak tissues can exacerbate this problem. The pressure of the pectoralis muscles can also squeeze the implants out to the side. Oftentimes the implant will not be just too far to the sides but low as well. It also seems to be more of a problem in patients with thin and weak tissue.
Years ago there was a belief that making a big pocket and having patients massage their breasts was a good way to reduce capsular contracture. It has since been learned that this is not correct. Yet some surgeons still do this, and if the pocket was made too wide then the implants can passively fall into that space.
When thin patients have a naturally wide and thin cleavage, their surgeons may put in excessively large implants in a futile effort to narrow their cleavage. However, when the tissues are thin and tight over the breastbone, they will squeeze the breast implant out to the side, thereby making the breast look worse because of the wide and bony gap between two unnaturally large implants. Nature does not make large breasts with wide gaps, so this condition can look very unattractive. In these cases, the problem is not a lateral malposition per se, but rather an overly large implant. Such patients must accept that a smaller implant is necessary to put their breasts into better proportion.
Lateral malposition can be fixed with a variety of techniques: a neosubpectoral or neosubglandular pocket, a capsular flap, acellular dermal matrix such as AlloDerm or Strattice, or reinforcement with a mesh such as Seri Scaffolding or Galaflex. The likelihood of a durable repair is very dependent upon the shape of the rib cage, the strength of the tissues, and the size of the implant. These patients very often have a rib cage that points outwards and so there may be some tendency for the breasts to be wide. Dr. Teitelbaum can discuss with you what he thinks is possible for you and what he expects to be able to achieve.